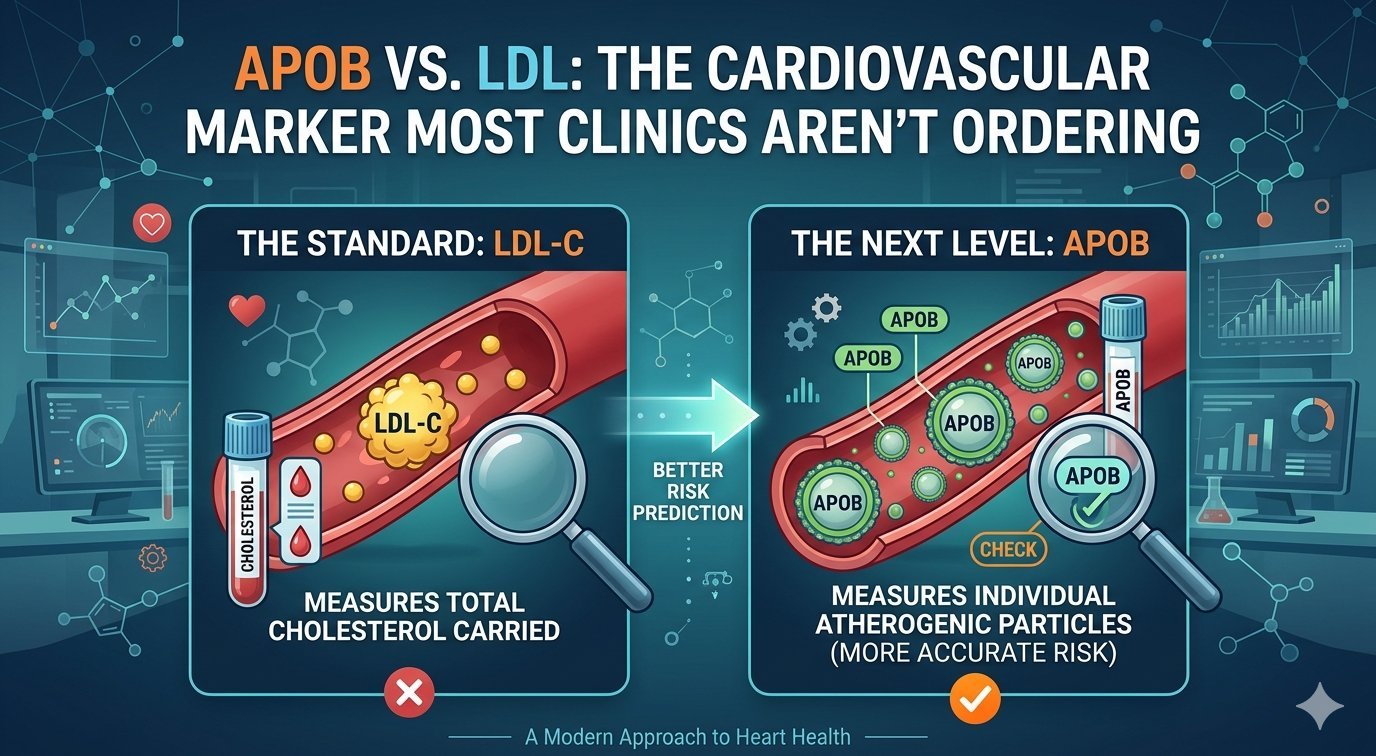
ApoB vs. LDL: The Cardiovascular Marker Most Clinics Aren’t Ordering
For five decades, LDL cholesterol has been the primary target of cardiovascular risk management. The problem: LDL is a concentration measurement, not a particle count. It is the number of particles — not the concentration of cholesterol within them — that most accurately predicts who will develop atherosclerosis. ApoB measures this directly.
By Aquiles Garcia-Menocal, APRN — Provena Care. Educational purposes only.
What Is ApoB?
Apolipoprotein B is a structural protein present — exactly once — on every atherogenic lipoprotein particle: every LDL, VLDL, IDL, and Lp(a) particle. Measuring serum ApoB gives you a direct count of the total number of atherogenic particles in your blood. This is particle number — what actually drives atherosclerotic plaque formation — not cholesterol concentration.
The Evidence for ApoB Over LDL
ApoB predicts cardiovascular events more accurately than LDL-C in multiple large studies including INTERHEART (27,000+ participants across 52 countries). Discordance between LDL and ApoB is common — 20–30% of patients have meaningfully discordant values, meaning their LDL underestimates actual particle burden. This discordance is particularly prevalent in patients with insulin resistance, metabolic syndrome, or a very low-carbohydrate diet.
How to Interpret Your ApoB Result
- Optimal: Below 80 mg/dL
- Near optimal: 80–99 mg/dL
- Borderline high: 100–129 mg/dL
- High: 130 mg/dL and above
At Provena, we target ApoB below 90 mg/dL for general prevention; below 70 mg/dL for patients with established cardiovascular disease, diabetes, or multiple risk factors. These targets reflect cardiovascular outcomes data — not population averages.
ApoB at Provena Care
ApoB is included in Performance and Elite lab panels. Core members can add it at member-preferred pricing. We also measure Lp(a) — a genetically determined lipoprotein with additional cardiovascular risk beyond ApoB — at baseline for Performance and Elite members. Most patients have never had Lp(a) measured.